
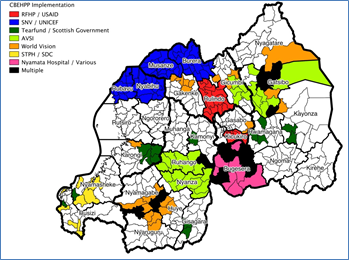
A recent workshop in Kigali hosted by Ministry of Health and supported by Unicef, USAID and Africa AHEAD provided all implemented partners with an update on how their contributions towards the Community Based Environmental Health Promotion Programme is enabling all villages in the country to be covered by this dynamic programme.
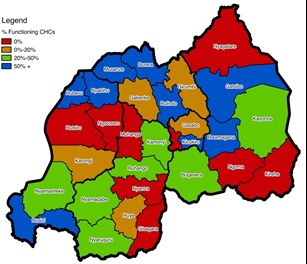
Over the past 5 years, since the initial launch of CBEHPP, many partners have been implementing CHCs to great effect and already 36% of all villages (5,376 out of 14,767) have so far benefitted from thorough CHC training, and this will be increased to 46% in the next year. However the balance till needs training and the good news is that Unicef has now committed to covering another 18 Districts, whilst USAID will cover 9 more districts. By the beginning of 2018, it is expected that every village in Rwanda will have a fully operational Community Health Club.
The information gathered at the workshop has provided some interesting new data on the cost of the programme, taking the data from the six main implementing partners. It is to be expected that there is some variation between the budget of different partners in CBEHPP, but cost per beneficiary even by the most generous budget does not go above US$5 per beneficiary.
Some development professionals have resisted using the CHC approach finding the model too complicated and imagining it is an expensive programme to implement given the design of 20 session for all members over a six month period. There is a tendency for international organisations to strive for innovation and a certain cynicism that the CHC Model if done in its text book form, can really predict a high level of behaviour change. They try to adjust the basic CHC model in tune with their own perceptions of what is cost-effective or desirable, providing the community with a miss mash of other approaches with often conflicting assumptions. To counter this MoH has been trying to coordinate the IPs and ensure a uniformity of the CHC Model across Rwanda.
The Gates Foundation in an effort to lay the debate to rest, has commissioned IPA (Innovations for Poverty Action) to do a Randomised Control trial to measure the cost effectiveness of the CBEHPP programme and two levels of implementation are being assessed, with result due next year:
- The Classic CHC Model as per the text book with all key aspects carefully included
- The ‘Lite’ version of the CHC Model which neglects one or more of the key aspects.
Training variations for Lite CBEHPP include:
- Training only CHFs without training SEHOs
- Smaller number of members
- Lack of use of membership card
- Reduced number of session to focus only on WASH subjects
- Reduced duration of training.
- Use of photocopied or b/w visual aids
- Reduced support for field workers
- Lack of monitoring with the household inventory
- Lack of certificates at the end of training
- Lack of transport for EHO and ASOC
Taking into account these possible variations of implementation, it has been found that the cost per CHC has an average of US$477 and ranges from US$76 to US$1,241; a factor of 16 times. Taking an achievable average of 80 members per CHC, it can be estimated that the cost per CHC Member is from US$0.95 to US$15. If each household is estimated at an average of 5 people, the cost per beneficiary drops to between 19c and US$3. This is considered cheap by any comparable standards.
Whilst the RCT trial will provide proper findings on the relative virtue of different levels of input we are encouraged to find that project records of a cross section of 6 major NGOs, reinforce our self proclaimed gold standard to provide health promotion and change hygiene behaviour at less than US% per beneficiary. It is helpful to know that our 5 x 5 Challenge to scale up reaching 5 million beneficiaries to address 5 killer diseases in 5 countries in the next 5 years at under US$5 per beneficiary) is in fact a realistic target.